A 21% surge in Covid-19 cases across Africa since early June casts spotlight on the SADC’s response to the pandemic
According to recent World Health Organization (WHO) reports, Covid-19 cases have be been steadily rising for five consecutive weeks since the onset of the third wave on 3 May 2021. “As of 20 June – day 48 into the new wave – Africa had recorded around 474 000 new cases, a 21% increase compared with the first 48 days of the second wave.” At the current rate of infections, the ongoing surge is set to surpass the previous one by early July. This has fuelled fears that the continent of 1.3 billion people may be unprepared and ill-equipped to adequately alleviate the impending threats posed by the third wave.
In anticipation of the third wave of the Covid-19 pandemic and the prevailing vaccine inequalities, particularly in Africa, it is essential to assess the state of readiness of the Southern African Development Community’s (SADC) member states response measures to the pandemic.
In a statement on January 2021, the SADC Chairperson, President Filipe Nyusi of Mozambique, encouraged a regional pooling of resources to facilitate procurement of necessary vaccines and distribution. However, this has been met with unforeseen challenges such as patent restrictions, unreliable supply of vaccines, and more wealthy nations hoarding vaccines at the expense of the Global South.
Since December 2020, several SARS-CoV-2 variants have been identified globally, in:
- the United Kingdom (B.1.1.7, also called Alpha),
- South Africa (B.1.351, also called Beta),
- Brazil (B.1.1.28, also called P1 or Gamma),
- United States (B.1.427/B.1.429, also called Epsilon) and I
- India (B.1.617, also called Delta).
So far, all but B.1.1.28 variant have been reported in Africa.
The WHO reclassified the highly contagious triple-mutant Covid variant spreading in India as a “variant of concern,” indicating that it’s become a global health threat. The first infections of the more transmissible Delta/B.1.617 variant had already been identified in Africa since the beginning of May 2021, further exacerbating fears that similar devastation seen in India may occur on the continent. Heightened transmissibility of the variant means more people can potentially become infected, which could ultimately result in more deaths for the non-vaccinated.
![]()
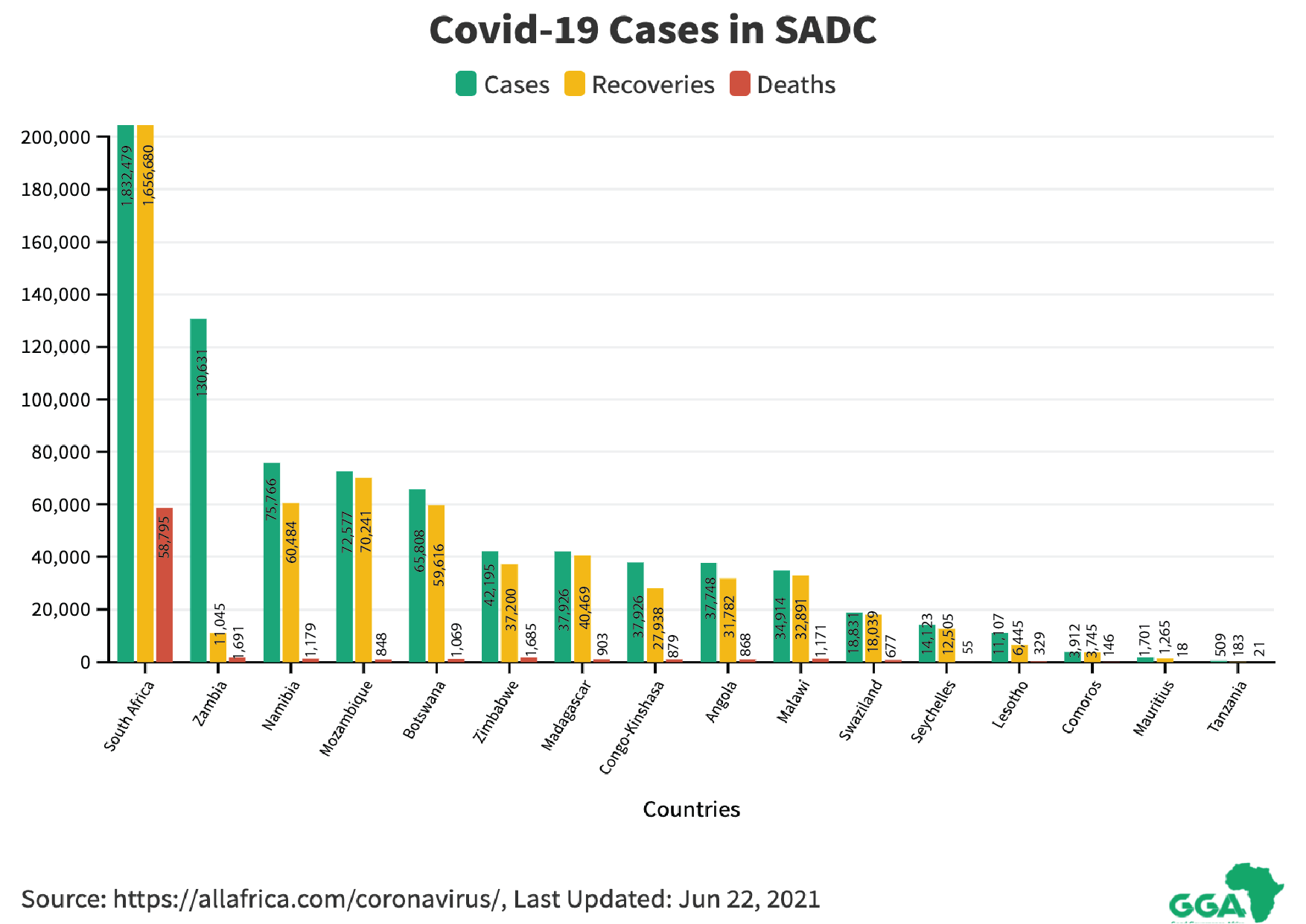
The majority of SADC countries, with the exception of Seychelles, have not had a large percentage of their population fully vaccinated, so have yet to reach herd immunity status.
The WHO has further highlighted that most African countries are running out of Covid-19 vaccines, and there are concerns about the future availability of vaccines. Globally, 150 doses of the vaccine have been administered per 1,000 people, but in sub-Saharan Africa it’s about eight doses per 1,000 people. To achieve herd immunity in the next 36 months in the SADC region, a country average of 100 000 vaccine doses per day need to be administered.
Regional response measures thus far
According to Dr Matshidiso Moeti, the WHO’s regional director for Africa, there is a need for a rapid roll out of the vaccine on the continent to strengthen its response measures to address the third wave of COVID-19. Moeti emphasised that Africa needs vaccines now and any pause in vaccination campaigns will lead to loss of lives and loss of hope. She continued by stating:
The third wave is picking up speed, spreading faster, hitting harder. With rapidly rising case numbers and increasing reports of serious illness, the latest surge threatens to be Africa’s worst yet. Africa can still blunt the impact of these fast-rising infections, but the window of opportunity is closing. Everyone everywhere can do their bit by taking precautions to prevent transmission.
In the SADC region, we have witnessed states at different stages of readiness as they prepare to battle the third wave. The following case studies highlight the range of response measures implemented by different SADC states:
Botswana
Botswana procured vaccines that are expected to cover over 50 percent of the population (1.9 million out of a total of 2.4 million people countrywide). While addressing a village leadership meeting in Toromoja, Vice President Slumber Tsogwane said 200 000 doses had already been received and that week, 88 907 people were vaccinated. The government has devised an initiative called “SmartBots” or” SmartBotswana”, which promote the use of technology in order to address challenges presented by COVID-19. In terms of vaccine capacity, Botswana could be the first SADC country to vaccinate its entire adult population.
The campaign of second dose of COVID-19 vaccines commenced on 8 June 2021. According to a press release from the Ministry of Health, it commenced with those who have received the Sinovac vaccine. Those who received the AstraZeneca vaccine will be due for their second dose in the week beginning 21 June 2021.
Democratic Republic of Congo
As the Democratic Republic of Congo (DRC) recovers from the effects of the eruption of Mount Nyiragongo on May 22, it has announced it is in the throes of the third wave of Covid-19. In a message on 3 June 2021, the Minister of Health announced: “Dear compatriots, the current situation of the Covid-19 pandemic in our country is very worrying. Indeed, there has been a considerable increase in cases and deaths in the past four weeks … I officially announce the occurrence of the third wave of the Covid-19 pandemic in our country, with the city province of Kinshasa as the epicentre.”
He indicated the reasons for the new surge in infections was due to:
- the relaxation of compliance with the Covid-19 protocol measures put in place
- the importation of cases following the movements of populations through their borders
- low vaccine coverage against the Covid-19
President Félix Tshisekedi expressed concern over the exponential upsurge in Covid-19 cases. He acknowledged that the situation “is very serious”, and that “the hospitals are saturated and there are many deaths”. Also, reports indicated that the Delta variant has been detected in most samples sequenced in the past month.
In addition, Tshisekedi has raised concerns about administering the AstraZeneca vaccine due to previously reported negative side effects and promised that the country would import other vaccines as well. He stated: “I had a meeting with those responsible for the response against Covid. During this meeting, the option of having a multitude of vaccines was floated. You know very well that the AstraZeneca vaccine posed some problems and continues to pose side effects. So, it would be better if we [get a variety] of vaccines.”
After more than a month of vaccine rollout, only 20,000 people have received the Oxford/AstraZeneca jab. Of those vaccinated, the majority are expatriates living in the country. The Congolese remain wary of the vaccine, and it appears poor communication from the government has worsened their fears.
Lesotho
The second phase of Lesotho’s mass Covid-19 vaccination programme was expected to begin on 16 June 2021. Those who had who received their first jabs of the AstraZeneca vaccine when the programme began in March will be eligible for their second dose. Those who did not receive the first vaccine shot will have to wait until after the country receives a different vaccine.
To mitigate the wait between vaccine shots, the government plans to switch to the Johnson & Johnson vaccine. The Health Minister Semano Sekatle recently stated they would procure Johnson & Johnson vaccines because “they present less logistical challenges as people only have to be vaccinated once.”
The launch of the second phase follows the delivery of 36 000 doses of the AstraZeneca vaccine donated by France. Minister Sekatle said Lesotho was expecting more vaccines from the African Union (AU) and a donation of over 100 000 vaccines from China. The arrival of more doses will enable more people to be vaccinated.
Lesotho received the first batch of AstraZeneca vaccines on 3 March 2021. The 36 000 doses enabled the government to roll out its mass vaccination programme a week later.
Malawi
By mid-May 2021, Malawi had received three batches of the AstraZeneca vaccine:
- 300 000 doses under COVAX
- 50,000 from India and
- 102 000 from the African Union
It was reported on 19 May 2021 that Malawi destroyed 17 000 expired AstraZeneca vaccines. The Malawi Health Minister, Kumbize Kandodo highlighted that despite their efforts of assurance and building faith in the vaccine, propaganda was to blame for the Malawian’s reluctance to receive the jab. Since the country launched its vaccination drive in March, it has inoculated only 300 000 people of its targeted 11 million by the end of the year (60 percent of the population).
Mozambique
The Covid-19 pandemic affected Mozambique at a critical time when the country was in the processes of infrastructure recovery and reconstruction from cyclones that were experienced two years ago.
Addressing a recent press conference in Maputo, the Deputy National Director of Public Health, Benigna Matsinhe announced that after three days without any deaths in Mozambique from Covid-19, the disease has claimed another victim. This brings the Covid-19 death toll to 838.
In February, Mozambique received 200,000 doses of Sinopharm. These doses, as is the norm across the region, were used in the first phase of Mozambique’s vaccination campaign, in which the priority group was healthcare workers.
In early March, the country received 484,000 doses of the Astra-Zeneca vaccine, produced in India. 384,000 doses were obtained through the COVAX initiative, and 100,000 were donated by the Indian government.
Last week, the Chinese military donated a further 60,000 vaccine doses. Although it is to be administered primarily to the Mozambican military, it is anticipated there will be sufficient doses to include some other groups of the population.
Also, some private companies have been authorised to import Covid-19 vaccines for their workers and their relatives. This is permitted on condition that the companies allocate 10 percent of their imported vaccines to the government.
Namibia
Recently, President Hage Geingob expressed his concern to the WHO that “vaccine apartheid” presented a growing risk of worsening the pandemic across Africa. Since then, he and First Lady Monica Geingos both tested positive for Covid-19. Reports have confirmed that as many as 527 learners and 165 teachers have tested positive for Covid-19 countrywide and are currently in isolation.
On Saturday, 30 May 2021 the Namibia Health Ministry reported that Namibia’s hospitals are full to capacity as the country battles a surge in COVID-19 cases. Namibia only has 166 high care and ICU beds countrywide for all patients, according to ministry figures. As a result the Ministry of Health has suspended non-emergency or non-urgent operations at two of its state hospitals with only emergency and urgent operations to be performed until further notice.
The Namibian Broadcasting Corporation’s (NBC) strike served as a major hinderance to the media broadcast vaccination campaign in Namibia. In April NBC workers went on strike for better salaries and working conditions. The announcement of meeting points and the overall vaccine education for the community were affected. The focal person for educating the community through the NBC Radio, Lebbeus Musongo (Kavango East and West regional health directorate) said that radio was the most effective means of communication to reach the audience in the remote inland areas where there are no newspapers, no internet or cell phones to keep them informed.
In a recent letter addressed to the Namibian Education Executive Director Sanet Steenkamp, the Teachers Union of Namibia (TUN) proposed that all schools remain closed for the rest of June and July 2021. TUN’s secretary general, Mahongora Kavihuha said that the proposal was driven by the alarming increase in Covid-19 cases among pupils and teachers.
Zimbabwe
Since February, Zimbabwe has received batches of COVID-19 vaccine from China, Russia and India. Four Covid-19 vaccines have been authorised by Zimbabwe:
- China’s Sinopharm and Sinovac vaccines,
- Russia’s Sputnik V,
- AstraZeneca from India.
In every crisis lies an opportunity. The slow vaccine rollout in several African countries has seen an increase in vaccine tourism to Zimbabwe. In an effort to be vaccinated, international travellers have been visiting Zimbabwe where private healthcare institutions administer the vaccine at reasonable costs. Since the vaccines offered in Zimbabwe are two dose shots, it means the travellers will have to return and boost the local economy in the process.
While Zimbabwe started off with a relatively good vaccination drive, the country has recently been facing shortages of COVID-19 vaccines despite the government’s push to inoculate at least 60 percent of the country’s estimated 14 million people by the end of the year. With regards to vaccine procurement, Information Minister Monica Mutsvangwa said 500,000 Sinopharm vaccine doses ordered from China are expected by June 2021.
In a recent development, the government has rejected Johnson and Johnson (J&J) vaccines from the African Union. The first allocation of J&J vaccines is set for August 2021. In a letter dated 2 June 2021, Secretary of Finance and Economic Development, George Guvamatanga said measures are still being put in place to establish the cold chain management framework for the vaccines:
The government of Zimbabwe notes that there is an allocation of the Johnson and Johnson vaccines due for August 2021. However, I wish to advise that the government of Zimbabwe is not yet ready to participate in the August allocation as measures are still being put in place to establish the cold chain management framework for the vaccines, as well as on management of the anticipated adverse effects of the vaccines following inoculation.
On 9 June 2021, Zimbabwe received its first consignment of 25,000 doses of Sputnik V, the Russian manufactured vaccine. It has been reported that the necessary measures are now in place for the shipment of the remaining 25,000 jabs.
Recently, Zimbabwean health and police officials have scaled up their surveillance measures in an attempt to curb the further spread of Covid-19 infections following a spike in hospital admissions while isolation centres are said to be fast filling up.
Due to the escalating Covid-19 infections, the government announced new lockdown regulations and placed Kadoma, Kwekwe, Hurungwe and Kariba on localised lockdowns, while other parts of the country were put under strict surveillance. The authorities anticipate more infections may lead to more medical attention sought and increased hospitalisation. There are also fears about the presence of the B.1.617 and B.1.351 variants, which have already been recorded in some parts of the country.
Recommendations for the SADC region
Combatting potentially deadly communicable diseases such as Coviid-19 is one of the founding objectives under SADC’s founding treaty and is also accounted for under the SADC Protocol on Health (1999). These recommendations highlight the importance of SADC countries doing everything in their power to better coordinate their efforts in order to meet the founding principles that are so obviously called for in this difficult time
Lessons can be learned from the case studies that could assist SADC states in their efforts to strengthen their response measures toward the Covid-19 pandemic:
- Timeous procurement of vaccines – has a positive effect on the rate of vaccines administered as highlighted in Botswana and Lesotho, both with relatively small populations, which have been more consistent and effective with a relatively well administered vaccine rollout.
- Expired vaccines – the expired vaccine episode in Malawi should be a warning to all states that adequate response measures should be in place before the arrival of a vaccine shipment as they do expire. SADC states are encouraged to fully capitalise on all available vaccines and to ensure mass vaccinations are carried out and avoid vaccines reaching expiration date.
- Collaboration between the state and private sector – Mozambique highlighted the benefits associated with collaboration between the state and the private sector. By allowing some companies to import the vaccine for their workers this freed up some of the procurement burden typically carried by the state. This may optimise the timeframe of the vaccine rollout in all SADC states.
- Media broadcast vaccination campaign – Namibia’s effective utilisation of their media broadcast vaccination campaign should be replicated across the region as radio stations are capable of reaching remote rural areas with limited internet connectivity.
- Diverse vaccine procurement – Zimbabwe has demonstrated the benefit of procuring vaccines from multiple suppliers. This approach has resulted in a larger number of people being vaccinated, with the available vaccines on hand at the time, and importantly eliminated the vaccination bottlenecks and delays in logistics/procurement.
- Vaccine tourism – Zimbabwe’s adaptiveness to benefit from vaccine tourism is an initiative that the other SADC states could explore if they have surplus supplies of vaccinations as long as vaccine tourism does not come at the expense of population-wide rollout.
- Transparency – also, Zimbabwe’s transparency in freely admitting the challenges it faces with regards to cold chain capacity creates an opportunity to formulate strategies to mitigate this limitation. SADC states should seek to formulate and implement mitigating strategies that will benefit and strengthen their response measures.
- Mass messaging – Continued communication and educating of all SADC citizens remains essential in addressing vaccine mistrust.
- Sustained vigilance – should continue as all gains made in combatting the pandemic thus far, could be wiped out. Studies have shown that the new variants are spreading more rapidly among younger populations, with evidence showing these newer variants, rather than just exploiting compromised immune systems, are showing some reactions in some younger healthy immune systems, resulting in severe inflammation and other serious symptoms.
- Preventative Covid-19 measures – continued importance of mask wearing and social distancing cannot be overstated. Prevention measures such as mask wearing, social distancing, and good hand hygiene are still as important as ever until vaccines become more readily available.
- Expanding and ramping up of vaccine rollout campaigns – must remain a priority for all SADC states the more people are vaccinated the safer the region will be in curbing the threat of the Covid-19 pandemic.
- Increase ICU capacity – this is the single most important variable in the fight against Covid-19. Avoiding hospitalisation should be key in formulating response measures.